

1 引言
手足口病(Hand, Foot, and Mouth Disease, HFMD)是全球关注的公共卫生问题之一,2008年被定为中国丙类传染病,是由A组71型(EV71)和柯萨奇病毒A组16型(CV16)等肠道病毒引起的常见传染病[1],多发生于5岁以下的婴幼儿[2],可引起发热和手、足、口腔等部位的皮疹、溃疡。HFMD病原体众多且彼此间共进化共循环,变异速度快,传播途径复杂,流行期隐性感染率高[3],若处理不当易造成集聚性爆发[4,5]。1957年新西兰最早报道了该病的流行,此后逐渐成为世界性的疾病[6]。根据中国疾病预防控制中心报告,近年来HFMD平均发病率达到了136例/10万[7],HFMD对婴幼儿身体健康造成严重威胁,给社会带来了巨大的医疗和保健负担。
国内外学者围绕HFMD的流行病学、临床表现、时空分布及发病的危险因素等开展了丰富的研究。最早关于HFMD的研究多集中在病原分析、诊断方法、发病机制、血清检测等方面[8]。近年来,地理学开始关注医学及健康的空间现象[9,10,11,12,13,14,15],有学者将HFMD发病的地理时空分布[16]、与环境因素的关系[17]及其病毒生境[18]纳入研究考量,从国家、省域[19]、县域[20]等尺度分析HFMD的季节特征[21,22]、发病周期[23]、空间集聚[24]和动态演变[25,26]。既有研究采用集中度及圆形分布法,分析发现中国HFMD呈现“夏秋季高发,两年为一周期”的发病规律[27,28,29];应用SaTScan回顾性时空扫描统计量、全局莫兰指数、Getis-Ord Gi*热点分析等方法,计算得到中国HFMD热点区集中在广西、广东、海南等南方湿热地区,北方大部分为冷点区[26, 29]。传染病流行的3个基本环节为传染源、传播途径和易感人群[30]。已有研究采用Logistic回归模型[31]、DLNM分布滞后非线性模型[32]、贝叶斯时空模型[33]、贝叶斯最大熵模型[34]、小波时间序列分析[35]等方法,发现HFMD的传染源为适合湿热环境繁殖的肠道病毒,主要受气温等自然环境因素影响[36],但对湿度、降水量、日照时数等其他自然环境因素的作用还存在分歧[16, 25, 37];HFMD的传播途径是密切接触和呼吸道飞沫传播,密切接触传播受人口密度和流动影响较大,空气质量差会加速呼吸道飞沫传播[38];HFMD的易感人群主要是5岁以下婴幼儿[30];传播途径和易感人群二者主要受社会经济因素影响[39]。综合而言,现有HFMD的研究虽然已经取得了一定进展,但对发病率的自然—社会—经济因素的综合影响尚缺乏可靠证据,基于市域中微观尺度研究全国范围内长时间序列的疾病时空分布还有待深入,需要构建地理学视角下自然科学和社会科学深度交叉耦合[40]的传染病研究理论框架。
基于此,本文对2008—2017年中国370个地级行政区HFMD发病率进行时空异质性分析,并以18个影响其发病的风险因子进行相关分析和地理探测,揭示其发病规律及传播机制,为地方疾控中心等相关部门开展HFMD防治、制定区域化防治策略、建立长效化防治机制提供理论支持和政策参考。
2 研究方法与数据来源
2.1 理论框架
传染病时空研究是一个由传染病发病的基本环节、影响因素和分布扩散状态[41]3个子系统构成的开放复杂巨系统[42],各子系统之间及子系统内部相互影响相互作用[43],共同构成健康地理学视角下传染病研究的理论框架(图1)。传染病发病的基本环节,是传染病得以发生的基础,由传染源、传播途径及易感人群三部分组成;影响因素,主要包括自然环境、社会经济和个体因素,能够促进或抑制基本环节的作用多寡或大小,不同因素影响不同的发病环节,传染源主要受自然环境及主观个体因素影响,传播途径主要受自然环境和社会经济因素影响,易感人群主要受社会经济及个体因素影响;分布及扩散状态,是影响因素作用于基本环节所呈现的疾病时空分布状态,主要指时间上的发病周期与规律、空间上的区域分布扩散状态及患病人群间的易感特征。由影响因素、基本环节到分布扩散状态,是科学研究从作用机理到表征的演绎过程;由分布扩散状态、基本环节到影响因素,则是从状态分析到原因解释的归纳过程;Logisitic回归、DLNM模型、贝叶斯模型、地理探测器等一系列数学或空间分析方法运用至实证案例研究,可以将3个子系统有机联结,进而探索发现三者有机关联的科学规律。
图1
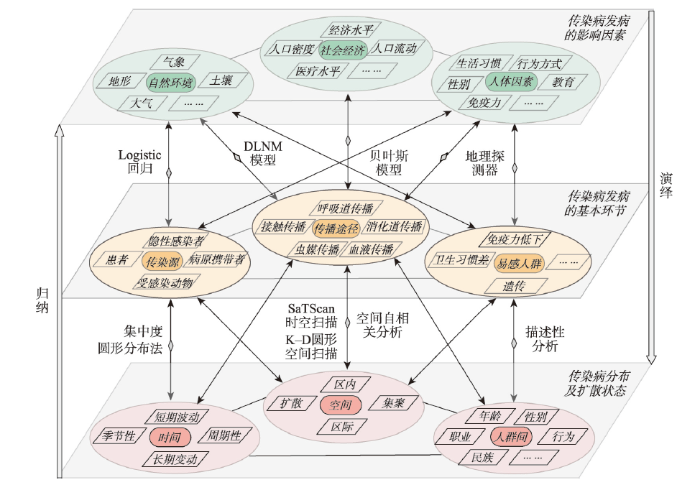
图1
健康地理学视角下的传染病研究理论框架
Fig. 1
Theoretical framework of infectious disease research from the perspective of health geography
本文基于该理论框架,选择性探究中国HFMD的时空分布特征及自然环境—社会经济双系统影响下的发病风险因素,暂未将发病的个体因素及在人群间的分布和扩散状态纳入研究内容。
2.2 指标体系
2.3 数据来源及预处理
本文选择中国31个省市自治区作为研究范围,以370个地级行政区(地级市、自治州、地区、盟、建设兵团)为基本研究单元,研究时段为2008—2017年共10年。发病率数据为中国地级行政区2008—2017年逐月HFMD发病率数据(港澳台未统计),来源于国家人口与健康科学数据共享平台正规申请数据(
表1 HFMD时空分异影响因素指标体系
Tab. 1
| 准则层 | 指标层 | 英文及简称 | 数据来源 |
|---|---|---|---|
| 自然环境 因素 | 海拔(m) | Digital elevation model, DEM | 资源环境科学与数据中心( |
| 年降水量(mm) | Annual precipitation, AP | 国家气象科学数据中心( | |
| 气压(hPa) | Barometric pressure, BP | 国家气象科学数据中心( | |
| 风速(m/s) | Weed speed, WS | 国家气象科学数据中心( | |
| 气温(℃) | Air temperature, AT | 国家气象科学数据中心( | |
| 相对湿度(%) | Relative humidity, RH | 国家气象科学数据中心( | |
| 日照时数(h) | Sunshine duration, SD | 国家气象科学数据中心( | |
| AQI指数 | Air quality index, AQI | 中国环境监测总站( | |
| 社会经济 因素 | GDP(亿元) | Gross domestic product, GDP | 中国城市统计年鉴 |
| 人均GDP(万元) | Per capita GDP, PCG | 中国城市统计年鉴 | |
| 一产占比(%) | Proportion of primary industry, PPI | 中国县(市)社会经济统计年鉴 | |
| 二产占比(%) | Proportion of secondary industry, PSI | 中国县(市)社会经济统计年鉴 | |
| 三产占比(%) | Proportion of tertiary industry, PTI | 中国县(市)社会经济统计年鉴 | |
| 城市化率(%) | Urbanization rate, UR | 中国城市统计年鉴、各省市统计年鉴 | |
| 千人床位数(张) | Hospital beds per 1000 persons, HBP | 中国县域统计年鉴(县市卷) | |
| 流动人口数(人) | Mobile population, MP | 流动人口数据平台( | |
| 人口密度(人/km2) | Population density, PD | 全球人口动态统计数据( | |
| 路网密度(km/km2) | Road network density, RND | 开放街道图( |
对全国各气象站点数据进行Kriging插值,得到全国31个省市自治区(港澳台未统计)、15 m左右空间分辨率的气象栅格图,再分区统计得到各地级行政区气象数据,其中日照时数、降水量为逐月求和数据,其余为年均数据;除气象因素外其他各因素均为全国31个省市自治区(港澳台未统计)的年份数据,其中人口密度和地形数据为1 km分辨率的栅格数据,采取分区统计并将值提取至各地级行政区的方法获取;路网密度数据为线状矢量数据,将路网图层与各地级行政区图层相交,再分类汇总得到各地级行政区的路网长度,与各区域总面积的比值即为路网密度;HFMD发病率数据与其他影响因素数据均与全国各地级行政区直接进行空间匹配得到。
2.4 模型及分析方法
2.4.1 集中度分析 集中度是分析HFMD各月份发病率在1年内的集中程度[47],公式为:
式中:ri表示某月HFMD发病率全年占比;i代表月份;Rx为x轴方向的离散度;Ry为y轴方向的离散度;M为集中度,取值范围为[0, 1],越趋于0表示发病情况在12个月中越均匀分布,越趋于1表示发病情况越集中在某1个月内。
2.4.2 空间自相关分析
(1)全局空间自相关
用全局空间自相关判定HFMD发病率在空间上是否存在集聚[48]。常用Moran's I来进行衡量,其取值为[-1, 1],大于0表示各地级行政区间存在空间正相关,小于0表示负相关,等于0表示不存在空间自相关性;绝对值越大表示相关性越强,即说明HFMD呈集聚分布形态。
(2)局部空间自相关
2.4.3 Spearman秩相关分析 采用Spearman秩相关分析来分析HFMD发病率与各影响因子之间的相关程度。该方法适用于非连续数据或变量总体分布未知的情况[51],考虑到影响HFMD发病率的各因素分布类型未知且多为非连续数据,故选用此方法来研究HFMD发病率与各因素之间的相关性。其计算公式如下:
式中:ri和si分别表示xi和yi的秩,当变量里出现相等值的时候,该值对应的秩为这几个值对应秩的平均值。rs的取值范围为[-1, 1],rs=1表示一个变量随另一个变量单调递增;rs=-1表示一个变量随另一个变量单调递减。
式中:q为影响因素对HFMD发病率的解释力大小探测指标;N为全国地级行政区数量;Nm表示m级地级行政区数量,m=1, …, n;n为影响因子的分类数;按照自然断裂点将各自变量自大到小分为5类,转化为类型变量。
表2 地理探测器交互作用类型及判别依据
Tab. 2
| 交互作用类型 | 判别依据 |
|---|---|
| 双因子增强 | q(X1∩X2) > Max[q(X1), q(X2)] |
| 非线性增强 | q(X1∩X2) > q(X1)+q(X2) |
| 非线性减弱 | q(X1∩X2) < Min[q(X1), q(X2)] |
| 单因子非线性减弱 | Min[q(X1), q(X2)] < q(X1∩X2) < Max[q(X1)), q(X2)] |
| 独立 | q(X1∩X2) = q(X1)+q(X2) |
3 结果分析
3.1 手足口病发病率时间变化特征
3.1.1 年度变化 2008—2017年全国各省HFMD年度发病率总体上呈现波动上升、两年为一周期且偶数年份高于奇数年份的发病规律(图2)。2008年为最低值,之后波动上升至2014年出现了统计年份的最高值,2014—2017年渐趋平稳,变幅不大。全国大部分省市发病率年度变化趋势基本一致,2014年都曾出现峰值,如包括广东省、广西壮族自治区和浙江省在内的大部分省份。相较于南方,北方各省份整体年份波动较小。个别省市变化特征出现异常,如海南省发病率在2011年出现明显增幅,远高于处于低发周期中的全国其他省份。
图2
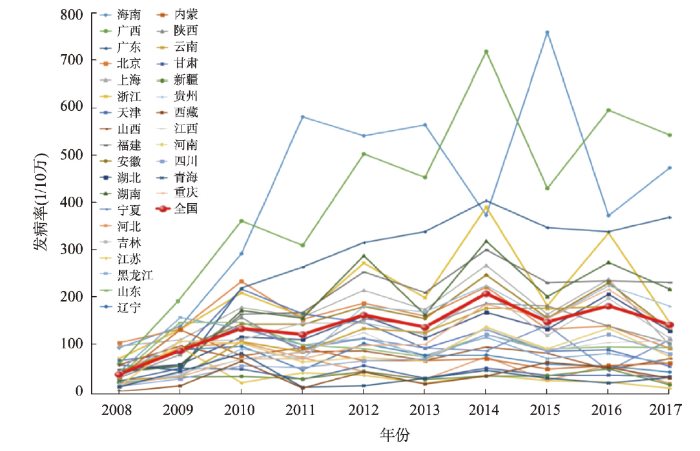
图2
2008—2017年中国HFMD各省年度发病率
Fig. 2
Annual incidence of HFMD in the provincial-level regions of China from 2008 to 2017
表3 2008—2017年中国HFMD发病率季节集中度
Tab. 3
| 年份 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
|---|---|---|---|---|---|---|---|---|---|---|
| 集中度 | 0.561 | 0.403 | 0.470 | 0.336 | 0.356 | 0.339 | 0.389 | 0.344 | 0.330 | 0.339 |
图3
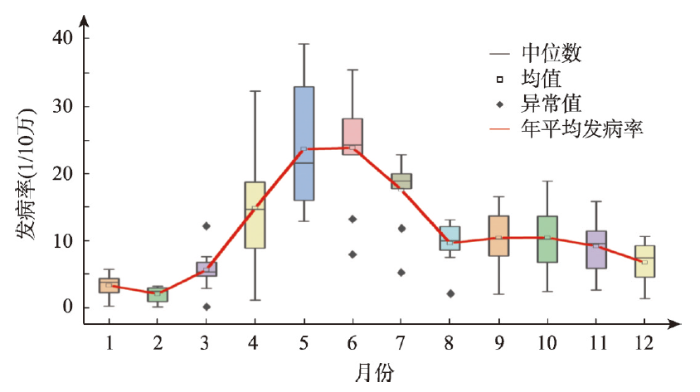
图3
2008—2017年中国HFMD各月份发病率箱线图
Fig. 3
Boxplot of monthly incidence of HFMD in China from 2008 to 2017
3.2 手足口病发病率空间集聚与分异特征
3.2.1 空间整体格局 2008—2017年全国HFMD发病率空间格局整体上存在明显的分异特征。2008年HFMD在全国大部分地级行政区均出现零星分布,个别西部偏远地区无数据。2009年全国HFMD发病率明显增加,京津冀地区、东北地区、山东半岛、长三角地区、珠三角地区HFMD发病率较高,而西部大部分地区HFMD发病率较低。2010—2017年全国HFMD发病率空间格局上趋于稳定;高发区域集中在南方大部分省份及经济较为发达的地区,如广西壮族自治区、广东省、海南省、北京市、上海市等;低发区域集中在胡焕庸线以西的大部分地区及东北地区,如西藏自治区、青海自治区、黑龙江省、吉林省等(图4)。
图4
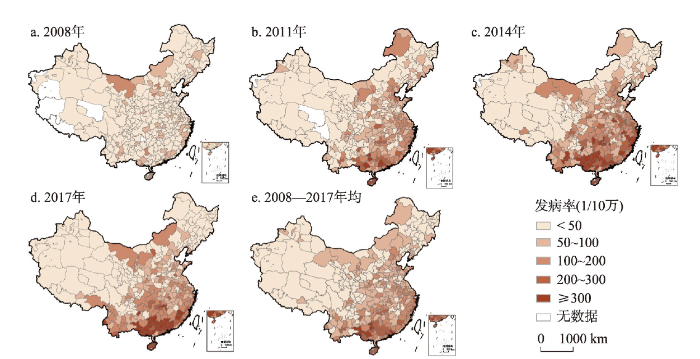
图4
2008—2017年中国HFMD发病率空间分布
注:基于自然资源部标准地图服务网站GS(2019)1825号标准地图制作,底图边界无修改。
Fig. 4
Spatial differentiation of HFMD incidence in China from 2008 to 2017
3.2.2 全局空间集聚性分析 2008—2017年HFMD发病率的Moran's I值均通过了显著性检验且Z值大于2.58,说明HFMD发病率呈现显著的空间集聚性(表4)。不同年份Moran's I从大到小依次为2015年(0.686)> 2017年(0.659)> 2013年(0.604)> 2011年(0.576)> 2012年(0.574)> 2014年(0.454)> 2016年(0.324),以上年份Moran's I大于0.3,较其他年份呈现集聚分布的空间格局。
表4 2008—2017年中国HFMD发病率的全局Moran's I分析结果
Tab. 4
| 年份 | Moran's I | Z值 | p值 | 空间格局 | 年份 | Moran's I | Z值 | p值 | 空间格局 |
|---|---|---|---|---|---|---|---|---|---|
| 2008 | 0.257 | 17.625 | 0.000 | - | 2013 | 0.604 | 44.679 | 0.000 | 集聚 |
| 2009 | 0.246 | 25.937 | 0.000 | - | 2014 | 0.454 | 33.834 | 0.000 | 集聚 |
| 2010 | 0.295 | 22.054 | 0.000 | - | 2015 | 0.686 | 50.786 | 0.000 | 集聚 |
| 2011 | 0.576 | 42.726 | 0.000 | 集聚 | 2016 | 0.324 | 24.201 | 0.000 | 集聚 |
| 2012 | 0.574 | 40.352 | 0.000 | 集聚 | 2017 | 0.659 | 46.008 | 0.000 | 集聚 |
注:p < 0.01表示相关性显著;“-”表示未体现明显的集聚分布。
3.2.3 局部空间集聚性分析 利用局部Getis-Ord Gi*热点探测来说明HFMD发病率的局部空间自相关特征,发现每一年度都存在HFMD发病率的地级行政区集聚区域,热点地区呈现自北向南,自小而分散向大而集中的分布趋势(图5)。2008年热点区较分散,主要分布在京津冀、长三角、珠三角等经济发达地区,冷点集中在中国西南地区。2009年热点区域明显增大,集中在华北平原大部分地区及珠三角小部分地区,冷点范围集中在西南部地区。2010—2017年发病率的冷热点分布趋于稳定,热点区域集中在广东省、广西壮族自治区及海南省,冷点集中在东北地区、华北地区、新疆西部及青海四川甘肃交界处的甘南藏区。
图5
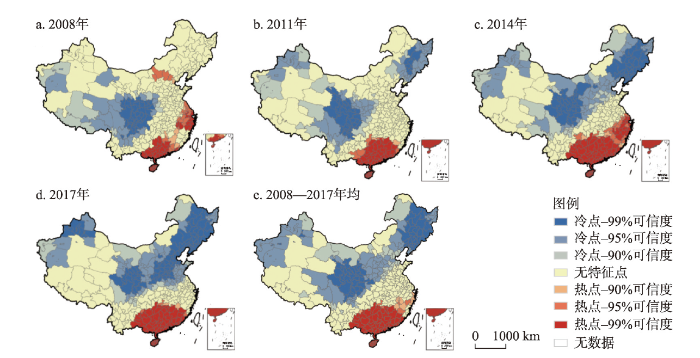
图5
2008—2017年中国HFMD发病率局部Getis-Ord Gi*分析结果
注:基于自然资源部标准地图服务网站GS(2019)1825号标准地图制作,底图边界无修改。
Fig. 5
Local Getis-Ord Gi* analysis of HFMD incidence in China from 2008 to 2017
3.3 手足口病发病率的影响因素
3.3.1 Spearman相关性分析 采用Spearman相关性分析方法得到中国各地级行政区HFMD发病率与影响因素的相关系数。由表5可知,除二产占比外其他17个影响因素均通过了0.05水平的显著性检验,其中气温与HFMD发病率的相关性最强达到了0.775,其次为降水量(0.734)、湿度(0.667),这3个因素与HFMD发病率呈现高度正相关。日照时数(-0.561)、风速(-0.434)、海拔(-0.382)、AQI指数(-0.319)与HFMD发病率呈较强的负相关关系。人口密度是社会经济因素中与发病率相关性最强的因素,达到0.389。相比之下,GDP(0.266)、千人床位数(-0.277)、流动人口(0.135)等社会经济因素与HFMD发病率相关性不强。
表5 2017年HFMD发病率与影响因素Spearman相关系数
Tab. 5
| 影响因素 | 相关系数 | 显著性 | 影响因素 | 相关系数 | 显著性 | 影响因素 | 相关系数 | 显著性 |
|---|---|---|---|---|---|---|---|---|
| 气温 | 0.775** | 0.000 | 海拔 | -0.382** | 0.000 | 一产占比 | -0.202** | 0.000 |
| 年降水量 | 0.734** | 0.000 | 气压 | 0.323** | 0.000 | 城市化率 | 0.178** | 0.000 |
| 湿度 | 0.667** | 0.000 | AQI指数 | -0.319** | 0.000 | 路网密度 | 0.160** | 0.000 |
| 日照时数 | -0.561** | 0.000 | GDP | 0.266** | 0.000 | 流动人数 | 0.135** | 0.000 |
| 风速 | -0.434** | 0.000 | 人均GDP | 0.232** | 0.000 | 三产占比 | 0.105* | 0.022 |
| 人口密度 | 0.389** | 0.000 | 千人床位数 | -0.227** | 0.000 | 二产占比 | 0.068 | 0.096 |
注:**表示p < 0.01,相关性显著;*表示p < 0.05,相关性较为显著。
3.3.2 地理探测器分析
(1)因子探测
用因子探测计算各个影响因素对HFMD发病率的影响强度(表6)。有12个影响因素通过了0.05水平的显著性检验。对HFMD发病率空间分异的解释力> 0.1的因子从大到小排序依次为气温(0.610)>降水量(0.506)>湿度(0.419)>日照时数(0.279)>风速(0.172)>AQI指数(0.160)>气压(0.108)>人口密度(0.103)。可以看出,自然环境因素对HFMD空间分异的的解释力相对较大,相比之下社会经济因素解释力较小。
表6 2017年影响因素对HFMD发病率的地理探测器解释力
Tab. 6
| 影响因素 | q值 | p值 | 影响因素 | q值 | p值 | 影响因素 | q值 | p值 |
|---|---|---|---|---|---|---|---|---|
| 气温 | 0.610** | 0.000 | 风速 | 0.172** | 0.000 | 路网密度 | 0.075* | 0.045 |
| 年降水量 | 0.506** | 0.000 | AQI指数 | 0.160** | 0.000 | 海拔 | 0.068** | 0.000 |
| 湿度 | 0.419** | 0.000 | 气压 | 0.108** | 0.000 | 千人床位数 | 0.067** | 0.000 |
| 日照时数 | 0.279** | 0.000 | 人口密度 | 0.103** | 0.004 | 人均GDP | 0.038* | 0.024 |
注:**表示p < 0.01,相关性显著;*表示p < 0.05,相关性较为显著。
(2)交互探测
利用交互探测器对HFMD发病率的影响因子进行交互探测,得到影响因子交互作用热力图及交互作用类型。由图6可知,气温与日照时数交互作用时对HFMD发病率解释力最强,达到了0.70,其次是气温与风速(0.68)、与年降水量(0.66)等其他各因子交互作用的解释力较强。相比之下,社会经济因素与自然环境因素交互作用时对发病率解释力一般,其中人口密度和气温交互作用时解释力最强,达到了0.66,其次是路网密度与气温(0.64)、千人床位数与气温(0.64)等双因子交互作用较强。社会经济因素两两之间交互作用均未通过显著性检验,说明影响HFMD发病率空间分异的主导因素是自然环境因素,其中气温、降水量与其他因子的交互作用对发病空间分异解释力最强。
图6
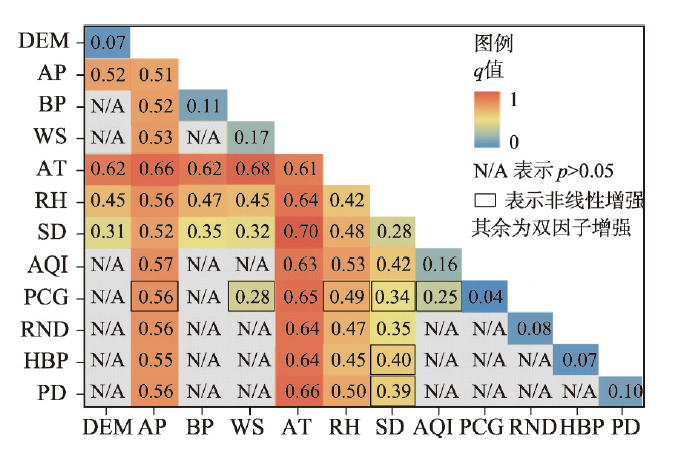
图6
2017年手足口病发病率影响因子交互作用热力图
Fig. 6
Interaction hotspot maps of factors influencing HFMD incidence in 2017
4 结果讨论
4.1 对时间变化结果的讨论
本文发现中国HFMD发病率呈现的周期性规律与前人结果基本一致[23]。但海南省发病率奇数年份高于偶数年份,其中2011年发病率远高于全国平均发病率,可能的原因在于2011年海南省内HFMD病例多由存活率高、致病率高的肠道病毒71型引起[52],该病毒通常会侵入神经和呼吸系统并引起急性神经和呼吸系统疾病[53],所以发病率高且产生的重症和死亡病例较多。此外,本文结果中HFMD发病呈现春季和秋季的双峰分布,与前人结果基本一致[29],这主要是由于中国季风性气候显著,春末夏初湿热天气促进了病毒的繁殖和扩散,另外也可能与学校假期时间有关,7—8月正值暑期学生互相分散能够降低发病率,而暑假结束进入秋冬季节,学校人群接触机会的增加导致发病风险增加,儿童对温度变化的适应性较差,也导致秋末冬初出现一个次高峰[54]。
4.2 对空间分布结果的讨论
本文HFMD发病率的缺失数据按空白处理,主要是考虑到发病率数据不具有自然连续属性,不宜进行插值。受地区发病上报率影响,缺失数据主要集中在2008—2015年新疆及西藏的西南部个别地区,可能对这些年份发病率空间分布结果造成一定影响,但缺失仅为个别现象对整体研究时段的结果影响不大。研究发现研究期早期HFMD发病率的热点地区主要分布在京津冀、长三角、珠三角等经济发达地区,冷点集中在西南地区,2011年之后发病热点集中在广西、广东等南方湿热地区,冷点集中在东北、华北及西北等干冷地区,验证了李颉等[26]的结果。这主要是因为前期HFMD上报率高的地区多为经济发达地区,随后全国各省份重视程度均有所提升上报率逐渐增多,加之南方地区湿热的环境更适宜病毒繁殖和传播,导致HFMD发病率的热点区域稳定集中在南方地区。
4.3 对发病率影响因素结果的讨论
本文仅研究2017年影响HFMD发病空间分异的因素,可能会造成部分研究结果的偏差,但全年份大区域无缺失的对应数据对分析影响因素的作用仍具有较强的说服力。综合考虑Spearman相关分析及地理探测结果,去除未通过相关分析和地理探测显著性检验的因素,有12项因素对HFMD发病空间分异有显著影响(图7)。气温、年降水量、湿度、日照时数、风速等5个因素,是上述两种方法分别得到的一致结果,且相关系数大小排序一致,说明其既与HFMD发病相关性最为强烈又是造成发病空间分异的最主要因素。依据Spearman相关分析所得影响因素的正负向及两种方法所得结果的对数趋势线对综合结果进行排序,与发病率体现正向作用的因素解释力从大到小依次为气温>年降水量>湿度>气压>人口密度>路网密度>人均GDP;负相关关系大小依次为日照时数>风速> AQI指数>海拔>千人床位数。其中,气温、降水量、湿度等因素与发病率呈正相关关系,这与龚胜生等[16]研究结果一致;风速与发病率呈负相关,与Wang等[36]研究结果一致;AQI指数与发病率呈负相关关系,可能原因在于虽然中国南方地区空气质量较北方地区更优良,但因受高温高湿的自然环境影响更显著,故AQI指数越低的地区发病率越高;气压与发病率呈正相关,与Zhang等[55]结果一致;人口密度、人均GDP等因素与发病率呈正相关关系,与Xu等[25]研究结果一致;路网密度与发病率呈正相关关系,与Hu等[35]研究结果一致。但本文发现日照时数与发病率呈负相关关系,与Song等[37]发现二者正相关的结果不一致,该学者采用日照时数单一因素与发病率做相关,在方法处理上与本文综合分析多因素得到的结论可能存在技术差异,加之日照可以增加紫外线强度并且从某种程度上也会减弱空气湿度,降低患病风险,负向相关可以解释;千人床位数与发病率呈现负相关关系,与丘文洋等[56]发现的山东省二者呈正相关的结论不一致,这可能与研究尺度不同、医疗水平差异和疾病上报率多少有关。本文虽是基于实测数据得到的统计学结果,但从病理学角度看,本文“高温高湿、多降水、少日照的地区发病率高”这一结果印证了“肠道病毒适合在湿热的环境下生存传播,但对紫外线和干燥敏感,自然光中的紫外线可直接破坏病毒的蛋白衣壳与核酸而使其灭活”[57]“自然因素通过影响人体免疫功能、人群生活模式来促进或抑制手足口病的发病”[58]及中医学中“手足口病多发于夏季,湿热病邪为主要病机,同时有湿和热双重特点”[59]的致病机理,可为传染病研究提供现实证据,具体病理原因还需不同专业背景继续做深入探讨。
图7
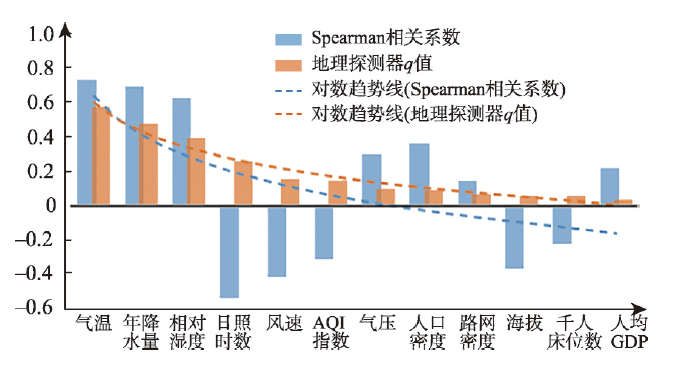
图7
HFMD发病空间分异影响因素
Fig. 7
Synthesis of two methods for influencing factors of spatial differentiation of HFMD
5 结论及展望
5.1 结论
HFMD严重威胁婴幼儿身体健康,引起多国政府和社会各界的广泛关注。本文采用全国范围内地级行政区传染病上报数据,研究中国手足口病发病率的时空分异特征及其影响因素。结论如下:
(1)构建了由传染病发病的基本环节、影响因素和分布扩散状态3个子系统构成的健康地理学视角下的传染病研究理论框架,各子系统之间及子系统内部相互影响相互作用,为传染病研究提供科学范式。
(2)2008—2017年全国HFMD发病率存在一定规律性,体现为波动上升、两年为一周期、偶数年份高于奇数年份的发病特点;季节性规律特点较鲜明,春末夏初为主高峰、秋末冬初为次高峰。
(3)2008—2010年HFMD发病率空间自相关特征不明显;2011—2017年发病率存在较强的空间自相关性且趋于稳定,发病热点地区呈现自北向南、自小而分散向大而集中的分布趋势,主要集中在广东、广西、海南等省份,发病冷点区集中在华北、东北、西北等北方干冷地区。总结手足口病多发区域,可以概括为于气候湿热区、经济落后且医疗水平低的地区及易集聚感染的人口密集区等三种典型地区。
(4)影响手足口病发病空间分异的地理要素主要有气温、年降水量、湿度、日照时数、风速、AQI指数、气压、人口密度、路网密度、海拔、千人床位数、人均GDP等 12个;与发病率体现正向作用的因素解释力从大到小依次为“气温>年降水量>湿度>气压>人口密度>路网密度>人均GDP”;负相关关系大小依次为“日照时数>风速>AQI指数>海拔>千人床位数”。其中,气温、湿度、降水量、日照时数、风速与发病率相关性及空间分异的影响作用最为强烈,印证了HFMD在湿热环境下的致病机理。各项因子之间的交互作用大于独自影响的作用,气温、降水量分别与其他因子的交互作用对发病空间分异的解释力最强。
5.2 研究展望
本文可为政府及其疾病控制中心等相关部门明确HFMD防治重点区域和重点环节提供科学依据:① 在春末夏初和秋末冬初两个高发期要做好对托幼机构、学校等重点场所HFMD日常防护的指导,提高儿童医院、传染病医院等医疗卫生机构对HFMD疫情的发现和处置能力;② 应针对不同地区特点制定区域化防治方案,重点关注中国南方湿热地区,尤其是广西、广东、海南等省份;③ 鼓励传染性疾病时空分异规律的探索研究,设立科学的疾病预警机制,可重点考虑气象条件中的气温、降水量、湿度、日照时数、风速等变量设计预警评估模型,持续做好疫情风险评估和提前防控。
本文理论框架构建尚未考虑传染病影响因素中的建成环境及城市形态等空间要素,且各要素构成空间特征的本身也暂未考虑;使用数据为地区上报HFMD发病数据,所在地的报告率、报告质量会对分析结果产生一定影响;此外,目前还缺少对连续年份影响因素及患者性别、年龄等人群特征方面的分析。未来,需要多学科对传染性疾病的地学理论框架做进一步补充和完善,并强化影响因素的空间转换;HFMD分地区分时段更为精细深入的分析、时空特征的病理解释、预警模型构建、健康风险评估及区划、及其与其他传染性疾病的胁迫影响分析,也将成为后续研究的重点。
致谢
中国疾病预防控制中心公共卫生科学数据中心提供数据支持。
参考文献
Emerging enteroviruses causing hand, foot and mouth disease, China, 2010-2016
DOI:10.3201/eid2410.171953 URL [本文引用: 1]
Trend analysis and forecast of daily reported incidence of hand, foot and mouth disease in Hubei, China by prophet model
DOI:10.1038/s41598-021-81100-2 URL [本文引用: 1]
The epidemiological risk factors of hand, foot and mouth disease among children in Singapore: A retrospective case-control study
Hand foot and mouth disease: Enteroviral load and disease severity
More cases of hand, foot, and mouth disease in China: A consequence of climate change
Global epidemic situation of hand, foot and mouth disease and molecular epidemiological research progress
全球手足口病流行现状及分子流行病学研究进展
Review on the epidemiology, etiology, and mechanism of infection of hand, foot, and mouth disease
手足口病流行病学、病原学及重症化机制的研究进展
Main progress and prospect of medical geography research in China
DOI:10.11821/xb199002008
[本文引用: 1]

The present paper related first, briefly the historical development of medical geography in China. During the period since 1960's, medical geography has got the greatest development. Es-pecially in the aspects of endemic diseases and cancers, the significant progresses have been made in studing geographical distribution law, geographical epidemic features, ecological charac-teristics, environmental pathogeny, environmental improvement and medical mapping. Based on the development of the discipline at home and abroad this paper briefly related the nature and task of medical geography. As a branch of geography or a marginal discipline, medical geog-raphy deals mainly with the laws of geographical distribution of diseases and health status in population, the occurrence, pathogenicity and endemic of diseases and variance of health status in relation to geographical environment, as well as the geographically rational disposition of health care system. According to the major research fields on medical geography (geography of diseases, geography of health, geography of health care, mapping of medical geography) their main achievements obtained in China have been expounded respectively. In geography of disease, following diseases are involved:1. The diseases related with biological factors in environment, plague, schistosomiasis, bru-cellosis and malaria;2. Those related with chemical factors in environment:(1) Se-abnormality disorders including Keshan disease, Kaschin-beck disease and end-emic selenosis;(2) Iodine abnormality disorders including endemic goitre and endemic cretinism;(3) Fluoride abnormality disorders including dental caries and fluorosis; 3. The mountain sickness related with environmental physical factors; and 4. Those with complicated pathogeniciity, such as cancers and cardiovascular diseases. As regards the health geography, some geographical features of life span, longevity region, st-ature and abnormal hemoglobin in China, are expressed in brief. With regard to snapping of medical geography, the major results obtained were the atlases of cancers, endemic diseases, schistisomiasis and aged population. Finally, this paper looked forward to the future of medic geography.
我国医学地理研究的主要进展和展望
A study on detecting multi-dimensional clusters of infectious diseases
DOI:10.11821/xb201204001
[本文引用: 1]
To indentify early signs of unusual health events is critical to early warning of infectious diseases. A new method for detecting multi-dimensional clusters of infectious diseases is presented in this paper. Ant colony clustering algorithm is applied to classify the cases of specified infectious diseases according to their crowd characters; then the cases belonging to the same class in terms of the space adjacency is separated; finally, the prior information about previous diseases outbreaks in the study area is applied to test the hypothesis that there was no disease cluster at various sub-regions. The detection ability of the method shows that this method does not need to accumulate case data within a long time period to detect irregular-shaped hot spots. It is useful for introducing spatial analysis to detection of infectious disease outbreaks.
传染病多维度聚集性探测方法
Overview on the research works in the field of environmental geography and human health
DOI:10.11821/yj2010090004
[本文引用: 1]
In the 1960s, the Institute of Geography called for chemical process research in physical geography and set up the first department on chemical geography in China. The department has participated in all earlier national programmes on environment, which has promoted the development of environmental sciences and technologies in China. The department also has led other institutes in the Chinese Academy of Sciences to conduct the studies on the geographic pathogeny and controlling of Keshan disease, Kaschin-Beck disease and other endemics, which has enhanced the initiation and development of medical geography in China. In 2000, the institute redistributed the department from chemical geography to environmental geography, as well as from medical geography to health geography. The expanding research works include the ecological and health risk assessment of pollutants such as heavy metals, the health risks of global environmental change, the biogeochemical cycles of carbon, nitrogen and their relationships with greenhouse gas emissions. Sets of technologies on site pollution treatment and health protection have been developed. Further research into environmental geography and human health will focus on the chemical property of geographic environment, so as to probe into the interactions among environment, human health and socio-economic development, for human safety and sustainable development.
环境地理与人类健康研究成果与展望
Trend and hot topics of medical geography
DOI:10.11820/dlkxjz.2013.08.011
[本文引用: 1]
In this paper, based on the discussions on the two main branches, ecological medical geography and health care geography, we reviewed current content and development process of medical geography. Through literature study and use of a software platform, we established a database which helps identify and rank citation rates, vocabulary frequencies, authors' countries and affiliations. We argued that, in contrast to classic literature, medical geography studies in recent years expanded the focuses from "disease" to "health" related geographical issues; research horizons expanded from global to national, to local, to neighborhood, and even to the inner space of a building; more and more research tools became available, and more and more spatial analysis methods have been used. The focuses of the studies of medical geography include: the impact of human development and socio-economic activities on health, spatial relationships between healthcare services, effects of healthcare behavior on the health conditions, the impacts of neighborhood environment, especially socio-economic conditions, health and healthcare equity issues, especially medical services and healthcare for the groups with special needs. The majority of the researchers are mainly from medical and public health fields, followed by the ones from geographic research institutions. Studies of medical geography are mainly in developed American and European countries, as well as the fast developing countries such as China, Brazil, and so on. This paper argued that research in medical geography should expand to a broader scope that includes the study of well-being; the spatial scale of the study would be widened, deepened, and expanded to the topics in virtual space such as online- base medical services; multidisciplinary researches would also be more widely adopted in the future.
医学地理学发展趋势及当前热点
Spatiotemporal characteristics and influencing factors of the epidemic disasters for the past 3000 years in China
DOI:10.11821/dlxb202108012
[本文引用: 1]
Epidemics are one of the most severe events in the human disaster network. On the basis of establishing the epidemic sequence by using historical epidemic data, and using the methods such as historical section analysis, factor correlation analysis, and time sequence analysis, this article examines the spatiotemporal characteristics and causes of the epidemic disasters for the past 2720 years (770 BC-AD 1949) in China. The results show that: (1) The frequency and intensity of epidemic disasters in China have a long-term upward trend, with troughs in the warm periods and peaks in the cold periods. (2) The epidemic prevalence in China generally occurred mainly in summer and autumn, but varied with time, so that since the 1450s, the seasonal difference tended to be less significant due to the increase of the kinds and frequency of epidemics. (3) China's epidemic fluctuation cycles are mainly 620-610 a, 320-310 a, 230-220 a, 170 a, 90 a, etc., which confirms the existence of "Twelve Earthly Branches" cycle and the significant impact of sunspot activity on the epidemic cycles. (4) For the past 3000 years, within the China's territory, the Epidemic Widespread is 93.51%, which indicates the percentage of the number of affected counties to the total number of counties, and the Epidemic Thickness is 16.86 layers, which represents the ratio of cumulative affected counties to the total number of administrative counties. The epidemics in the southeast half of China occurred much more frequently and severely than those in the northwest half. (5) The expansion of the epidemic prevalent areas in China is synchronized with the areal land exploration. The change of the epidemic centers of gravity is obviously affected by the spatial changes of the economic centers of gravity. The centers shifted from north to south before the Southern Song Dynasty, and moved from east to west after that. The import of foreign infectious diseases has a great impact on the distribution pattern of epidemics in China. (6) The prevalence of epidemics is not only a natural phenomenon, but also a sociocultural phenomenon. The change in the spatiotemporal distribution of epidemics reflects the change of human-environmental relationship. The densely populated areas, the areas along the traffic line, the surrounding areas of the capital city, the natural foci areas and the disaster-prone areas are all epidemic-prone areas. (7) The geographical environment has a basic impact on the spatial distribution of epidemics, that is, low altitude, warm and humid areas are prone to the prevalence of epidemics. Natural disasters can induce epidemics, so the disaster-prone area is also the epidemic-prone area, and the disaster-prone period is also the epidemic-prone period. Climate change has impacts on epidemic fluctuations, so epidemics are more frequent in the cold periods than in the warm periods. The land excessive development and the conflict between human and land resulting from population growth intensified the epidemic prevalence. Moreover, epidemics always follow wars, that is, the frequent periods of war are also the frequent periods of epidemic.
中国3000年疫灾流行的时空特征及其影响因素
A research framework of precise epidemic prevention and control from the perspective of Space-time Behavioral Geography. Scientia Geographica Sinica
新冠肺炎疫情精准防控的时空间行为地理学研究框架
Health geography II
DOI:10.1177/0309132515581094 URL [本文引用: 1]
Geographical characteristics and influencing factors of the prevalence of hand, foot and mouth disease in Hubei Province
湖北省手足口病流行的地理特征及其影响因子
Effect of climatic factors on hand, foot, and mouth disease in South Korea, 2010-2013
Study on spatiotemporal evolution of hand, foot and mouth disease in China under the influence of meteorological factors
气象因素影响下中国HFMD时空演化特征研究
Detecting spatial-temporal cluster of hand foot and mouth disease in Beijing, China, 2009-2014
DOI:10.1186/s12879-015-1330-0 URL [本文引用: 1]
Application of distributed lag non-linear model in the research of influence of meteorological factors on hand foot and mouth disease
分布滞后非线性模型在气象因素对手足口病发病影响研究中的应用
Epidemiological analysis, detection, and comparision of space-time patterns of Beijing hand, foot and mouth disease, 2008-2012
Study of the epidemiology and etiological characteristics of hand, foot, and mouth disease in Suzhou City, East China, 2011-2014
DOI:10.1007/s00705-016-2878-8
PMID:27146138
[本文引用: 1]
Hand, foot, and mouth disease (HFMD) is a common childhood illness that is caused by enteroviruses, and the prevalence of HFMD in China and around the world has resulted in a huge disease burden. Since 2010, the HFMD incidence has been the highest among infectious diseases in Suzhou, China. To investigate the epidemical, features, etiological characteristics, and clinical characteristics of HFMD in Suzhou City, East China, from 2011 to 2014. We retrospectively analyzed HFMD epidemiological data in Suzhou from 2011 to 2014. A total of 80,723 outpatients in the city of Suzhou were diagnosed with HFMD, including 1,846 severe cases. There were 2,387 (3.0 %) laboratory-confirmed cases, 807 of which exhibited severe symptoms. All analyses were stratified by age, disease severity, laboratory confirmation status, and enterovirus subtype. From 2011 to 2014, HFMD mainly affected children aged 1-3, and boys were more affected than girls. The highest peak incidences of HFMD occurred in May or June from 2011 to 2014, and lower peak incidences were observed from November to December and in districts with higher humidity. Enterovirus 71 and coxsackievirus A16 were the predominant viral genotypes in Suzhou in 2011 to 2012 and 2014, and the severe cases mainly correlated with EV71 subtypes. In 2013, other EVs were dominant. The proportion of patients with severe disease decreased significantly, and the VP1 capsid proteins of EV71 and CA16 from severe and mild cases were nearly identical. This study shows that it is time to start monitoring EVs in China and that we should accelerate vaccine research and develop public-health interventions for the control and prevention of HFMD, all of which will play an important role in the prevention of HFMD.
Epidemic situation and coping strategies of HFMD
手足口病的流行概况和应对策略
The epidemic features of the hand, foot, and mouth disease during 2008-2011 in China
2008—2011年中国大陆手足口病流行特征分析
Spatio-temporal pattern and risk factor analysis of hand, foot and mouth disease associated with under-five morbidity in the Beijing-Tianjin-Hebei region of China
DOI:10.3390/ijerph14040416 URL [本文引用: 3]
Spatial-temporal heterogeneity of Hand, Foot and Mouth Disease in China from 2008 to 2018
2008—2018年中国手足口病时空分异特征
Application of concentration and circular distribution method to explore the epidemic law of HFMD in Henan Province in 2010
应用集中度和圆形分布法探讨河南省2010年手足口病流行规律
Circular Statistics in Biology
Surveillance of hand, foot, and mouth disease in Mainland of China (2008-2009)
DOI:10.3967/0895-3988.2011.04.005
PMID:22108323
[本文引用: 3]
Since HFMD was designated as a class C communicable disease in May 2008, 18 months surveillance data have been accumulated to December 2009. This article was to describe the distribution of HFMD for age, sex, area, and time between 2008 and 2009, to reveal the characteristics of the epidemic.We analyzed weekly reported cases of HFMD from May 2008 to December 2009, and presented data on the distribution of age, sex, area and time. A discrete Poisson model was used to detect spatial-temporal clusters of HFMD.More than 1 065 000 cases of HFMD were reported in Mainland China from May 2008 to December 2009 (total incidence: 12.47 per 10 000). Male incidence was higher than female for all ages and 91.9% of patients were <5 years old. The incidence was highest in Beijing, Shanghai, Zhejiang and Hainan. The highest peak of HFMD cases was in April and the number of cases remained high from April to August. The spatial-temporal distribution detected four clusters.Children <5 years old were susceptible to HFMD and we should be aware of their vulnerability. The incidence was higher in urban than rural areas, and an annual pandemic usually starts in April.Copyright © 2011 The Editorial Board of Biomedical and Environmental Sciences. Published by Elsevier B.V. All rights reserved.
HFMD Guidelines for Diagnosis and Treatment (2018 Edition)
手足口病诊疗指南(2018年版)
Construction of HFMD epidemic prediction model and screening of severe risk factors
[D].
手足口病流行预测模型的构建及重症危险因素筛选
[D].
Study on the influence of air temperature on the incidence of HFMD based on the nonlinear model of distribution lag
[D].
基于分布滞后非线性模型的气温对手足口病发病率的影响研究
[D].
Space-time variability and determinants of hand, foot and mouth in Shandong province: A bayesian spatio-temporal modeling approach
利用贝叶斯时空模型分析山东省手足口病时空变化及影响因素
Hand, foot and mouth disease: Spatiotemporal transmission and climate
DOI:10.1186/1476-072X-10-1 URL [本文引用: 1]
Transmission center and driving factors of hand, foot, and mouth disease in China: A combined analysis
Detecting the association between meteorological factors and hand, foot, and mouth disease using spatial panel data models
DOI:10.1016/j.ijid.2015.03.007 URL [本文引用: 3]
Exploring spatiotemporal nonstationary effects of climate factors on hand, foot, and mouth disease using Bayesian Spatiotemporally Varying Coefficients (STVC) model in Sichuan, China
DOI:10.1016/j.scitotenv.2018.08.114 URL [本文引用: 3]
Short-term effect of El Niño: Southern oscillation on pediatric hand, foot and mouth disease in Shenzhen, China
Thinking clearly about social aspects of infectious disease transmission
DOI:10.1038/s41586-021-03694-x URL [本文引用: 2]
Drivers of PM2.5 air pollution deaths in China 2002-2017
DOI:10.1038/s41561-021-00792-3 URL [本文引用: 1]
Geographies of Health: An Introduction
Disciplinary structure of geographic science in China
DOI:10.11821/dlxb202109001
[本文引用: 1]
The modern international and domestic science advancements have brought forward new opportunities as well as higher requirements to the development of geographic science in China. In planning the disciplinary structure of geographic science in the "Development Strategy of Discipline and Frontier Research in China (2021-2035)", we propose a modified disciplinary structure for the geographic science in the new era. The geographic science in China can be categorized into four secondary disciplines, i.e., integrated geography, physical geography, human geography, and information geography, considering the current situation and development outlook of geographic science. The tertiary disciplines under each secondary discipline are nearly fully developed, and a few quaternary disciplines under tertiary disciplines have already been widely accepted and used. We hope this new disciplinary structure can play a breakthrough role for improving the branches of geographic science, promoting the development of emerging disciplines under the framework of geographic science, and better serving the international and domestic development needs in the new era.
中国地理科学学科体系浅析
Geodetector: Principle and prospective
DOI:10.11821/dlxb201701010
[本文引用: 2]
Spatial stratified heterogeneity is the spatial expression of natural and socio-economic process, which is an important approach for human to recognize nature since Aristotle. Geodetector is a new statistical method to detect spatial stratified heterogeneity and reveal the driving factors behind it. This method with no linear hypothesis has elegant form and definite physical meaning. Here is the basic idea behind Geodetector: assuming that the study area is divided into several subareas. The study area is characterized by spatial stratified heterogeneity if the sum of the variance of subareas is less than the regional total variance; and if the spatial distribution of the two variables tends to be consistent, there is statistical correlation between them. Q-statistic in Geodetector has already been applied in many fields of natural and social sciences which can be used to measure spatial stratified heterogeneity, detect explanatory factors and analyze the interactive relationship between variables. In this paper, the authors will illustrate the principle of Geodetector and summarize the characteristics and applications in order to facilitate the using of Geodetector and help readers to recognize, mine and utilize spatial stratified heterogeneity.
地理探测器: 原理与展望
Environmental health risk detection with GeogDetector
The effect of temperature on childhood hand, foot and mouth disease in Guangdong Province, China, 2010-2013: A multicity study
The proof and measurement of association between two things
DOI:10.1093/ije/dyq191 PMID:21051364 [本文引用: 1]
Comparison between general Moran's Index and Getis-Ord gerneral G of spatial autocorrelation
全局空间自相关Moran指数和G系数对比研究
Quantile local spatial autocorrelation
DOI:10.1007/s12076-019-00234-0 URL [本文引用: 1]
The analysis of spatial association by use of distance statistics
DOI:10.1111/gean.1992.24.issue-3 URL [本文引用: 1]
Simulating comparisons between Spearman and Kendall's tau-b methods for the nonparametric bivariant correlation analysis
非参数双变量相关分析方法Spearman和Kendall的Monte Carlo模拟比较
Hand, foot, mouth, brainstem, and heart disease resulting from enterovirus 71
DOI:10.1097/CCM.0b013e318291cb2d URL [本文引用: 1]
Epidemiological characteristics of HFMD in Huishan District of Wuxi City from 2012 to 2016
[D].
2012—2016年无锡市惠山区手足口病流行病学特征分析
[D].
Space-time heterogeneity of hand, foot and mouth disease in children and its potential driving factors in Henan, China
A bayesian network method considering spatial cluster to valuate health risk of hand, foot and mouth disease
利用空间聚集的贝叶斯网络评估手足口病发病风险
Guidelines for prevention and control of hand, foot and mouth disease (2009 Edition)
手足口病预防控制指南(2009 版)
Virology, epidemiology, pathogenesis, and control of enterovirus 71
DOI:10.1016/S1473-3099(10)70194-8
PMID:20961813
[本文引用: 1]
First isolated in California, USA, in 1969, enterovirus 71 (EV71) is a major public health issue across the Asia-Pacific region and beyond. The virus, which is closely related to polioviruses, mostly affects children and causes hand, foot, and mouth disease with neurological and systemic complications. Specific receptors for this virus are found on white blood cells, cells in the respiratory and gastrointestinal tract, and dendritic cells. Being an RNA virus, EV71 lacks a proofreading mechanism and is evolving rapidly, with new outbreaks occurring across Asia in regular cycles, and virus gene subgroups seem to differ in clinical epidemiological properties. The pathogenesis of the severe cardiopulmonary manifestations and the relative contributions of neurogenic pulmonary oedema, cardiac dysfunction, increased vascular permeability, and cytokine storm are controversial. Public health interventions to control outbreaks involve social distancing measures, but their effectiveness has not been fully assessed. Vaccines being developed include inactivated whole-virus, live attenuated, subviral particle, and DNA vaccines.Copyright © 2010 Elsevier Ltd. All rights reserved.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}