
西藏自治区层级医疗设施可达性精细化评价
|
刘泽(1998-), 男, 湖北武汉人, 硕士生, 主要从事健康地理学研究。E-mail: 202021051051@mail.bnu.edu.cn |
收稿日期: 2022-08-29
修回日期: 2023-04-22
网络出版日期: 2024-02-01
基金资助
第二次青藏高原综合科学考察研究(2019QZKK0406)
Refined assessment of accessibility to hierarchical health care facilities in Xizang
Received date: 2022-08-29
Revised date: 2023-04-22
Online published: 2024-02-01
Supported by
The Second Tibetan Plateau Scientific Expedition and Research Program(2019QZKK0406)
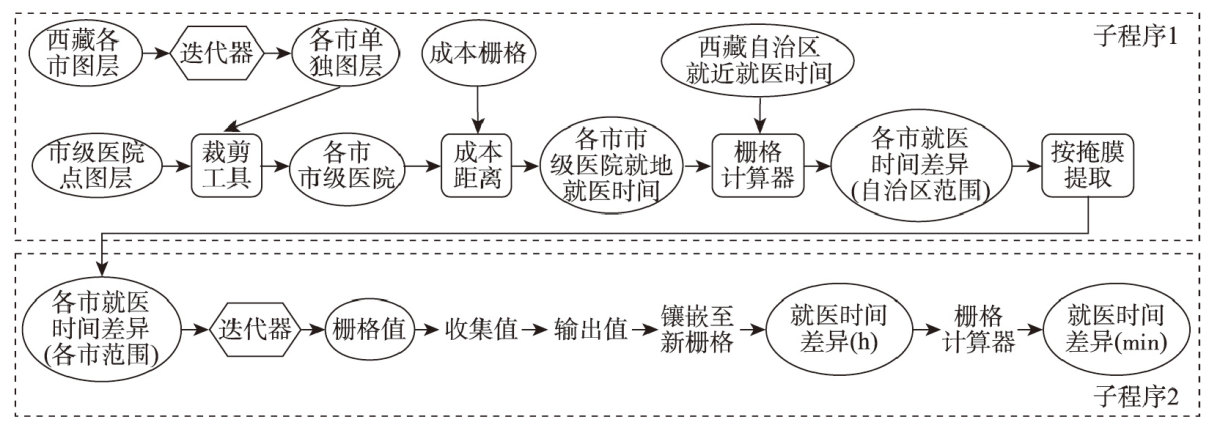
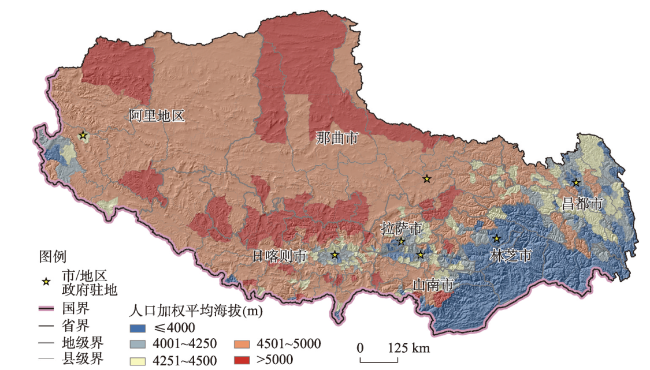
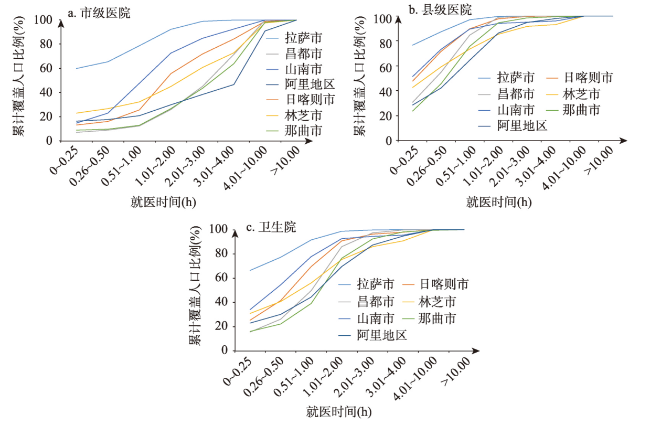
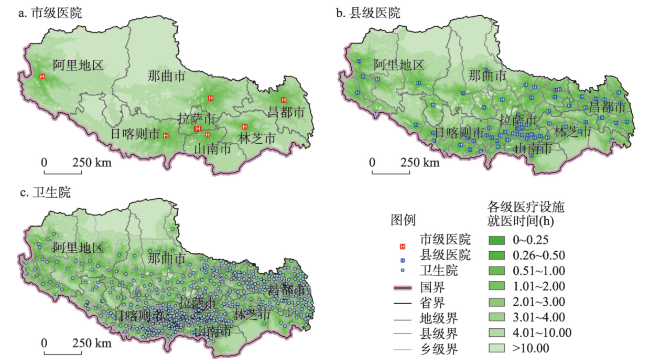
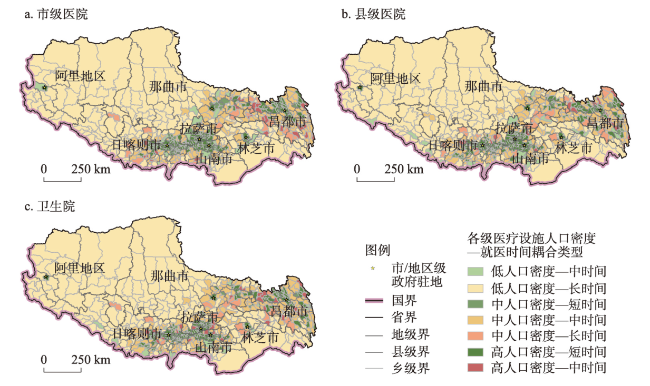
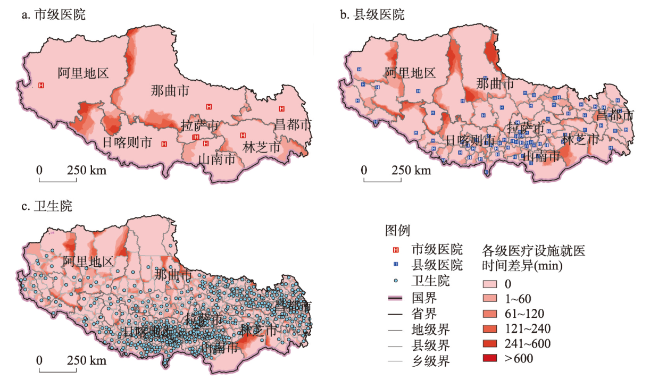
西藏自治区地处青藏高原,地理环境独特,精细化评价该地区医疗设施可达性对于促进医疗服务均等化具有重要的现实意义。本文使用西藏自治区地形和高程等自然地理数据、土地利用、路网、医疗设施以及人口数据,在1 km×1 km栅格尺度精细化评价各级医疗设施的就医时间,统计不同就医时间段内覆盖的人口比例,识别缺医区,并评价就近就医和就地就医方式下可达性的空间差异,为优化西藏医疗设施的配置提出建议。结果表明,西藏市级医院、县级医院和卫生院在1 h内分别可覆盖36.01%、65.55%和86.54%的人口,低等级医疗设施的覆盖人口比例较高。通过人口密度与就医可达性的耦合分析,识别出的缺医区主要位于那曲市与昌都市。就近就医与就地就医方式存在可达性差异的地区主要位于山南市与林芝市,建议在政策上促进这些地区居民跨行政区就近就医便利化。本文建立了适用于青藏高原医疗设施可达性精细化评价的方法框架,并系统评价了西藏自治区医疗设施可达性格局,为促进医疗服务均等化提供科学依据。
刘泽 , 程杨 , 陶卓霖 , 孔劲松 . 西藏自治区层级医疗设施可达性精细化评价[J]. 地理学报, 2024 , 79(2) : 502 -514 . DOI: 10.11821/dlxb202402013
The Xizang Autonomous Region is located in the Qinghai-Tibet Plateau and has a unique geographical environment. The refined assessment of the accessibility to health care facilities in the region is of great practical significance for promoting the equalization of health care services. This study applies the geographical data of Xizang, such as data on topography and elevation, land use, road networks, health care facilities, and population, for refined assessment of the travel time to the hierarchical health care facilities at the 1 km×1 km grid scale. The proportion of population covered by different time periods of travel time to health care facilities is evaluated and the health care shortage areas are identified. In addition, the spatial differences between proximity-based and administrative district-based accessibility to health care facilities at each level are evaluated in order to provide suggestions for optimizing the locations of health care facilities in Xizang. The results show that the proportion of population traveling to municipal hospitals, county-level hospitals, and health centers within one hour at the township level in Xizang is 36.01%, 65.55% and 86.54%, respectively. The proportion of population covered by low-level health care facilities is higher than that of the high-level health care facilities within one hour. By applying coupling analysis of population density and health care accessibility, the identified health care shortage areas in Xizang are mainly located in Nagqu and Qamdo. The areas with differences between proximity-based and administrative district-based accessibility to health care facilities are mainly located in Shannan and Nyingchi. Therefore, policies should be suggested to promote the convenience of local residents accessing the nearest health care facilities by crossing the administrative boundaries. This study establishes a methodological framework for the refined evaluation of health care accessibility in the Qinghai-Tibet Plateau, systematically evaluating the spatial pattern of accessibility to health care facilities in Xizang so as to provide scientific evidence for promoting the equalization of health care services in the region.
表1 道路速度及影响因素系数Tab. 1 Road speed and the coefficient of influencing factors |
| 道路分类 | 速度赋值 (km/h) | 平均纵坡 (%) | 坡度影响 系数 | 高程 (km) | 高程影响 系数 | 用地类型 | 用地类型影响 系数(%) |
|---|---|---|---|---|---|---|---|
| 高速公路 | 100 | ≤ 10 | 1 | ≤ 3 | 1 | 城市建设用地 | 100 |
| 一级公路/主干道 | 80 | (10, 20] | 0.95 | (3, 4] | 0.95 | 草地 | 95 |
| 二级公路 | 60 | (20, 30] | 0.9 | (4, 5] | 0.9 | 裸地 | 80 |
| 三级公路 | 30 | (30, 50] | 0.7 | (5, 6] | 0.7 | 灌木 | 70 |
| 无道路 | 20 | (50, 100] | 0.4 | (6, 7] | 0.4 | 林地、农田 | 65 |
| > 100 | 0.1 | > 7 | 0.1 | 湿地、雪地 | 30 | ||
| 水体 | 0 |
表2 2020年西藏自治区各级医疗设施不同时间阈值内覆盖人口比例(%)Tab. 2 The proportion of population covered by health care facilities at each level within various travel time thresholds in Xizang in 2020 (%) |
| 0~0.25 h | 0.26~0.50 h | 0.51~1.00 h | 1.01~2.00 h | 2.01~3.00 h | 3.01~4.00 h | 4.01~10.00 h | >10.00 h | |
|---|---|---|---|---|---|---|---|---|
| 卫生院 | 47.16 | 19.39 | 19.99 | 10.07 | 1.95 | 0.47 | 0.97 | 0.00 |
| 县级医院 | 32.94 | 12.06 | 20.55 | 22.69 | 7.49 | 2.32 | 1.93 | 0.04 |
| 市级医院 | 23.27 | 3.54 | 9.20 | 18.12 | 13.97 | 13.13 | 17.79 | 0.99 |
表3 2020年西藏各地市级医院前往西藏自治区人民医院所需时间Tab. 3 The travel time from municipal hospitals to the People's Hospital of Xizang in 2020 |
| 市级医院 | 前往所需时间(h) |
|---|---|
| 拉萨市人民医院 | 0.20 |
| 西藏自治区第二人民医院 | 0.40 |
| 西藏自治区第三人民医院 | 0.42 |
| 山南市人民医院 | 1.82 |
| 日喀则市人民医院 | 3.58 |
| 那曲市人民医院 | 4.61 |
| 林芝市人民医院 | 5.65 |
| 昌都市人民医院 | 12.69 |
| 阿里地区人民医院 | 18.70 |
表4 2020年西藏人口密度—可达性耦合类型下乡/镇/街道个数占比(%)Tab. 4 The proportion of townships by various coupling types between population density and health care accessibility of Xizang in 2020 (%) |
| 低人口— 中时间 | 低人口— 长时间 | 中人口— 短时间 | 中人口— 中时间 | 中人口— 长时间 | 高人口— 短时间 | 高人口— 中时间 | |
|---|---|---|---|---|---|---|---|
| 市级医院 | 2.90 | 30.04 | 3.63 | 25.83 | 3.34 | 29.75 | 4.50 |
| 县级医院 | 3.77 | 29.17 | 2.47 | 26.12 | 4.21 | 30.91 | 3.34 |
| 卫生院 | 2.61 | 30.33 | 3.19 | 26.56 | 3.05 | 30.19 | 4.06 |
表5 2020年西藏总体及高海拔与边境地区人口加权就医可达性Tab. 5 The population weighted accessibility to health care facilities of Xizang, the areas with high altitude and border regions of Xizang in 2020 |
| 市级医院(h) | 县级医院(h) | 卫生院(h) | |
|---|---|---|---|
| 总体 | 2.27 | 0.92 | 0.50 |
| 人口加权平均海拔> 4500 m | 3.52 | 1.40 | 0.73 |
| 人口加权平均海拔> 5000 m | 4.71 | 2.64 | 1.69 |
| 边境 | 5.50 | 2.07 | 1.54 |
表6 2020年西藏各级医疗设施就近与就地就医可达性差异区域的面积与人口占比Tab. 6 The proportion of areas and population with differences between proximity-based and administrative district-based accessibility to health care facilities at each level in Xizang in 2020 |
| 市级医院 | 县级医院 | 卫生院 | |
|---|---|---|---|
| 面积占比(%) | 13.24 | 22.68 | 25.87 |
| 人口占比(%) | 12.16 | 14.23 | 20.82 |
| 人口加权就医时间差异(min) | 3.54 | 5.03 | 3.77 |
| [1] |
[新华社. “健康中国2030”规划纲要. 2016. https://www.gov.cn/zhengce/2016-10/25/content_5124174.htm.]
|
| [2] |
The State Council of the People's Republic of China. China Rural Poverty Alleviation and Development Program (2011-2020). 2011. https://www.gov.cn/gongbao/content/2011/content_2020905.htm.
[国务院. 中国农村扶贫开发纲要(2011—2020年). 2011. https://www.gov.cn/gongbao/content/2011/content_2020905.htm.]
|
| [3] |
[蔡岷, 李方平. 西藏统计年鉴. 北京: 中国统计出版社, 2021: 273-284.]
|
| [4] |
[杨雯丽, 陈能, 王慧敏, 等. 基于改进2SFCA上海中心城区医疗设施可达性研究. 地理信息世界, 2020, 27(6): 75-79.]
|
| [5] |
[扆运杰, 赵君, 李熹, 等. 基于GIS的医疗设施布局及空间可达性研究: 以北京市Z区为例. 中国卫生政策研究, 2021, 14(6): 66-71.]
|
| [6] |
[柳泽, 杨宏宇, 熊维康, 等. 基于改进两步移动搜索法的县域医疗卫生服务空间可达性研究. 地理科学, 2017, 37(5): 728-737.]
|
| [7] |
[郭亮, 彭雨晴, 贺慧, 等. 分级诊疗背景下的武汉市医疗设施供需特征与优化策略. 经济地理, 2021, 41(7): 73-81.]
|
| [8] |
[王东华, 曹小曙, 黄晓燕. 中国集中连片特困地区医疗可达性对贫困的影响. 陕西师范大学学报(自然科学版), 2021, 49(2): 2-14.]
|
| [9] |
[霍青兰, 唐新明, 王鸿燕, 等. 六盘山地区医疗设施空间分布及可达性研究. 测绘科学, 2021, 46(7): 189-195.]
|
| [10] |
[刘振, 刘盛和, 戚伟, 等. 青藏高原流动人口居留意愿及影响因素. 地理学报, 2021, 76(9): 2142-2156.]
|
| [11] |
[王楠, 王会蒙, 杜云艳, 等. 青藏高原人口流入流出时空模式研究. 地理学报, 2020, 75(7): 1418-1431.]
|
| [12] |
[许珺, 徐阳, 胡蕾, 等. 基于位置大数据的青藏高原人类活动时空模式. 地理学报, 2020, 75(7): 1406-1417.]
|
| [13] |
[高兴川, 曹小曙, 李涛, 等. 1976—2016年青藏高原地区通达性空间格局演变. 地理学报, 2019, 74(6): 1190-1204.]
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
Health Commission of Xizang Autonomous Region. Implementation Plan of Tibet Autonomous Region on Further Deepening the Construction of Compact County Medical Community. 2021.
[西藏自治区卫生健康委员会. 西藏自治区关于进一步深化紧密型县域医共体建设的实施方案. 2021.]
|
| [21] |
[王振波, 徐建刚, 朱传耿, 等. 中国县域可达性区域划分及其与人口分布的关系. 地理学报, 2010, 65(4): 416-426.]
|
| [22] |
[汪延彬, 何瑞东, 王娅妮, 等. 基于成本距离的铁路客运站交通可达性空间特征研究: 以甘肃省为例. 安徽师范大学学报(自然科学版), 2022, 45(1): 58-63, 77.]
|
| [23] |
[苗毅, 卢文清, 戴特奇, 等. 青藏高原市域综合交通优势度评价及空间特征: 以林芝市为例. 地理科学进展, 2021, 40(8): 1332-1343.]
|
| [24] |
|
| [25] |
Department of Finance of Xizang Autonomous Region, Health Commission of Xizang Autonomous Region. Measures on Rewards and Subsidies for Special Positions of Township Health Centers in High Altitude Areas. 2017. https://www.tibetol.cn/html/2017/xizangyaowen_0527/31801.html.
[西藏自治区财政厅, 西藏自治区卫健委. 关于高海拔地区乡镇卫生院专业技术人员特殊岗位奖励补贴办法. 2017. https://www.tibetol.cn/html/2017/xizangyaowen_0527/31801.html.]
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}